Key points
- You’re at a higher risk of skin cancer after transplant because your medications make you more sensitive to the sun.
- You need to protect your skin at all times, even on a cloudy day and in all seasons.
- You should do a full body check each month to spot any new or changing lesions. You will also get an annual full body check by a dermatologist.
- There are certain signs to look out for, that indicate a lesion might be cancerous.
Why you are at risk
As a transplant recipient, you are at higher risk of developing certain skin cancers due to your immunosuppressive medications. While these are essential, they affect the immune system's ability to prevent the development of abnormal cells such as cancer. In fact, lung transplant patients are more susceptible to skin cancer after transplant, compared to other organ transplant recipients.
Some medications can cause photosensitivity reaction, which means your skin is more sensitive to sunlight. You will burn more easily, which increases the risk of developing aggressive skin cancers like squamous cell carcinoma (SCC). This applies for the following medication:
- Septrin®
- common antibiotics such as Doxycycline and Ciprofloxacin
- some antifungal medications such as Voriconazole
- some blood pressure medication such as Amlodipine and Nifedipine
You need to use higher skin protection with these drugs and inform your doctor if you have a reaction.
“Within 5 years of having a transplant, 1 in 20 patients will have developed skin cancer. By 10 years, 1 in 10 will.”
- Dr Patsy Lenane, Dermatology Consultant
Your risk of developing skin cancer is even higher if you:
- have fair skin, lots of freckles, blue or green eyes, red or blonde hair
- work or spend a lot of time outdoors
- have used sunbeds in the past
- have a prior history of actinic keratosis (pre-cancers) or skin cancer
- were over the age of 65 when you had your transplant
- have been on intense immunosuppression medications for a long time
Checking your skin
- Be on the lookout for any new markings or spots on your skin.
- Complete a full skin check each month. Have a look at your entire skin surface, using 2 mirrors. If you need help, ask one of your care partners.
- You should have a full body skin check with a dermatologist every year. These will be scheduled through the transplant clinic.
Visit your GP (or your dermatologist, if you have one) if you notice any new or changing lesions on your skin, especially ones that are increasing in size, bleeding, painful or not healing. Do not wait until your next clinic appointment. The earlier skin cancer is found, the easier it can be treated.
“Remember to check your skin regularly and if in doubt, don’t delay, get it checked. Do NOT wait until your next appointment.”
- Dr Patsy Lenane, Dermatology Consultant
What to look out for
Here are some examples of lesions that are either cancerous or pre-cancerous.
Melanoma (cancer)
Melanomas can occur anywhere on the skin, including the back, soles of the feet and on other hard-to-see areas. Melanoma often looks like a brown or black mole or birthmark. However, it often stands out as looking different to your other moles. Sometimes melanoma can be pink or red so if you have any new or changing lesions you should have it reviewed by a dermatologist.
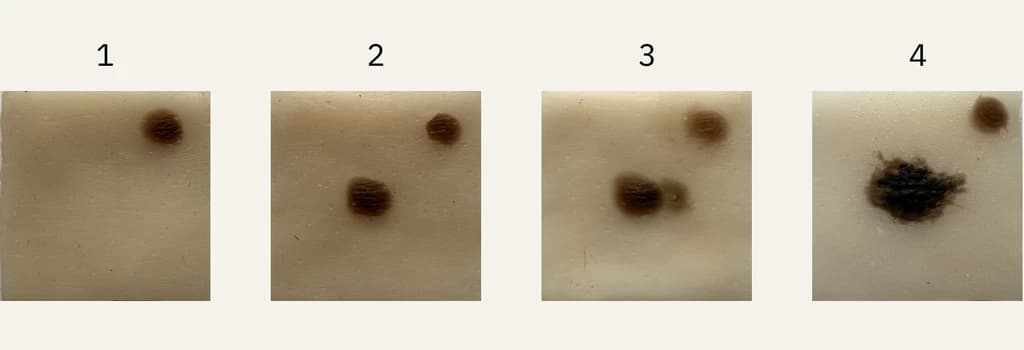
Progression model of melanoma
- Existing mole - Watch out for new moles.
- New mole - Keep an eye for any changes.
- Changing mole - Mole is changing in colour, shape or size.
- Advanced changes - Mole is changing further in colour, shape or size.
Actinic keratoses (AK) to squamous cell carcinoma (SCC)
Some people, especially those with fair skin, can get scaly, rough, or bumpy spots called 'actinic keratoses'. They are often found on the face, ears, arms, or scalp. There is a very low risk that these areas may develop into a skin cancer. Your GP or dermatologist can treat actinic keratosis with a cream or freeze treatment.
SCCs are much more common in patients who have had an organ transplant compared to the general population. They often show up as a new, firm lump that may be scaly, tender or bleeding. The most common places are on the scalp, face, neck and back of the hands.
It is important to recognise these early and see a dermatologist. They can be surgically removed or radiotherapy is an alternative treatment option for larger lesions. It’s important to get treatment quickly.
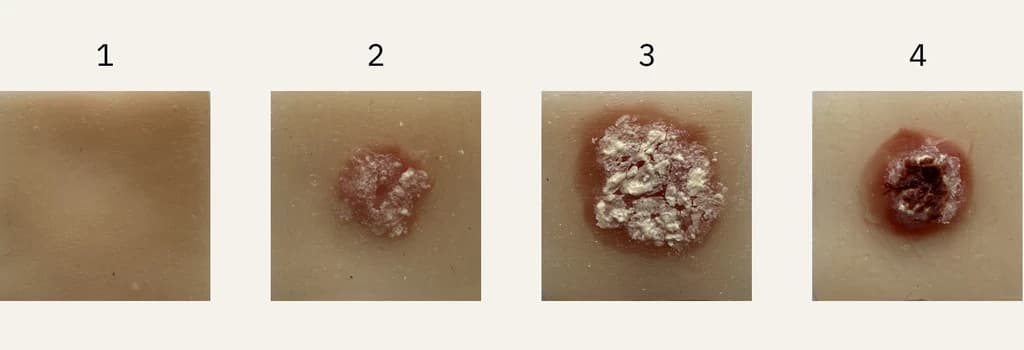
Progression model of SCC
- Sun damage - Watch your skin.
- Severe sun damage - Keep an eye for any changes.
- Larger raised area - Seek medical help.
- Open sore - Seek medical help.
Basal cell carcinoma (BCC)
BCC is a common type of skin cancer that often appear as a sore or crusted area that may bleed occasionally and does not heal completely. They usually show up on areas of the skin that are exposed to the sun, such as your head and neck. If left untreated, a BCC can erode the skin and cause an ulcer. A dermatologist or plastic surgeon can treat a BCC by surgically removing it. It is important to know that they do not spread to other parts of the body beyond the skin.

Skin model of Basal Cell Carcinoma (BCC)