Key points
- In ICU, you will have several tubes, drains and monitoring devices in place to support your breathing, nutrition and recovery.
- You may need additional temporary procedures, such as bronchoscopies, ECMO or a tracheostomy.
- Close monitoring helps the team to detect complications early, such as new infection or rejection.
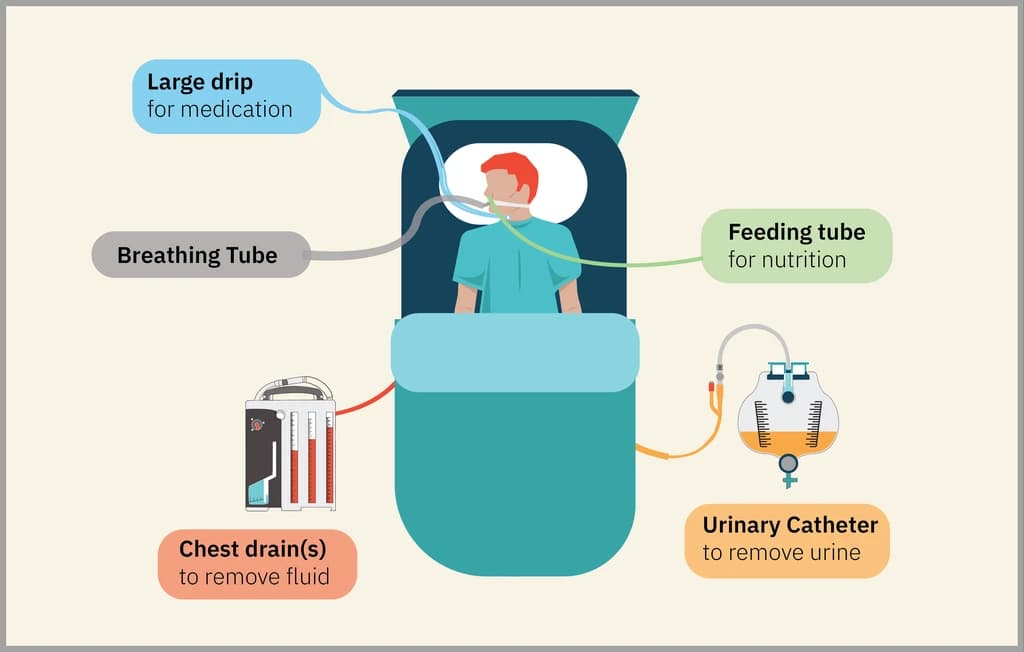
Drains and tubes
When you arrive to the ICU, you'll have lots of drains and tubes in place.
Wounds and scars
After your surgery you will have a wound along your breastbone, directly below and across your ribcage. It will be covered by a dressing to keep the wound clean while it heals.
Bronchoscopy
We regularly perform a procedure with a catheter attached to a camera called 'bronchoscopy' to look into your lungs. We will do this in the ICU, to make sure that the internal post-surgery scars on your lung(s) look good and to rule out infection. You will need to be put to sleep to get this procedure done. We always do it when you have an empty stomach to avoid an aspiration pneumonia (infection caused by food getting into the lungs).
During the bronchoscopy, we will take samples from inside your lungs to make sure you are on the correct treatment. You will be on specific antibiotics during the surgery and for up to 2 weeks after transplant. However we may learn after surgery that the donor had an infection we weren't aware of and we may need to change your antibiotics accordingly.
When you are immunosuppressed, you at higher risk of getting infections. We will need to stay on top of this. You will be scheduled for surveillance bronchoscopies as an outpatient when you leave the hospital. This will be done to make sure you do not have any infection. We also take a sample of tissue to rule out a form of rejection called acute rejection. We will talk to you about this as you are preparing for discharge.
ECMO
During the surgery, the team may use ECMO (extracorporeal membrane oxygenation) to replace the function of your lungs while the new lung(s) are inserted.

Your privacy settings
In order to allow the use of this content on this website you must accept the use of miscellaneous cookies.
The team will aim to remove the ECMO machine at the end of surgery. However, there is a chance that the new lungs may not work well enough at first, and may need more time to recover. If this happens, the surgeon and anaesthetist may decide to leave you connected to the ECMO machine for longer. This allows your lungs to rest and gives them time to recover from the surgery. If this happens you will be transferred to ICU on ECMO where the staff are trained to care for you while you receive this support.
It is also possible that the new lungs may struggle for hours or even days after surgery. In this case, you may need to be placed on ECMO after you return to ICU. This can often be done by the intensive care team at the bedside, or you may need to return to the operating theatre to have the procedure done there.
While ECMO can provide clinical stability, it comes with risks. Once on ECMO, you will be assessed every day by the transplant and intensive care teams. When your lungs have recovered well enough, the ECMO machine will be removed.
The most common risks of ECMO are:
Tracheostomy
Some patients may need help with their breathing for a longer period of time after their transplant. In this case, the ICU and transplant team may consider a tracheostomy. This is a small plastic tube that is inserted into the trachea (windpipe) through an opening in the front of the neck. This is temporary and will be removed when your strength and lung function has recovered. A tracheostomy tube is more comfortable than the breathing tube placed in your mouth. It helps you to gradually come off the ventilator, to clear secretions (like mucus or phlegm) from your lungs and to allow you to gradually increase your mobility, even if your lungs still need some support.
If you have a tracheostomy, you will not be able to use your voice at first, but over time as you gain strength, your voice and ability to eat and drink will gradually come back. Until this happens, your nurse and speech and language therapist will help you to communicate using a whiteboard or a picture communication board to point toward. When you are strong enough, the speech and language therapist will add a speaking valve to the tracheostomy tube so that you can start using your voice again.
The tracheostomy is used until you can breathe on your own and are strong enough to clear your own chest secretions. The time required varies with each patient but can take weeks or even months. When your team decides the tracheostomy tube is no longer required, the tube will be removed at your bedside and the tiny hole in the front of your neck will close over in a few days.
Potential complications
It is common to experience setbacks in your recovery, particularly in the early days and weeks after transplant. We will be monitoring your condition very closely, so we can detect and manage any complications as early as possible. It is impossible to predict what specific challenges you might face but some of the more common complications include the following.
Rejection
Rejection is where your body doesn’t recognise the new lung(s) as your own and so attacks it, trying to 'reject' them from your body. To limit the risk, the team will start you on your immunosuppressant medications at the time of surgery. The team will monitor you very closely. Rejection can usually be managed successfully if it is picked up early.
To learn more, go to Risk of rejection.
Infection
There is a risk of infection after any surgery. This risk is much higher after transplant surgery because the medications you receive to stop your body rejecting the new lung(s) will weaken your ability to fight infection.
We will start you on antibiotics at the time of the surgery to reduce the risk of infection. If we suspect you have an infection, we may take blood or urine samples and consider changing the lines we use to give you medications. As the lungs are a common source of infection, we may carry out bronchoscopies regularly to monitor for infection.
To learn more, go to Risk of infection.
Kidney problems and dialysis
Sometimes the kidneys may not work normally after a transplant. This can be caused by many things including major surgery and medications. If this is severe, we may need to use a dialysis machine to help clear the toxins from your blood and prevent your body from holding onto too much fluid. We hope this will be temporary and that your kidneys will recover over time. Unfortunately not everyone’s kidneys recover. There is a small chance you may require dialysis permanently. This is more likely in patients with prior kidney disease, low blood pressure or those who had significant bleeding during the surgery.
Diabetes
You will need regular blood sugar checks as patients often develop diabetes after transplant due to the immunosuppression. If you did not have diabetes before, it may just be short term. However it is possible that you will develop permanent diabetes. This is most common for patients that were ‘borderline’ or ‘pre-diabetic' before the transplant. This means they had higher than normal blood sugar, but not high enough to be diagnosed as diabetic. In this case you would then need to take medications, including possibly insulin, for life. This carries another set of rules and will require close monitoring by the diabetes team to get it under control.